")
")







The Institute for Neurosciences of Montpellier (INM) is the Joint Research Unit U1298 Inserm/University of Montpellier. It comprises 8 Inserm teams and a staff of 200 personnel working on sensory-motor deficits and neurodegeneration. INM aims to gather fundamental and translational research to study the development, synaptic plasticity and integration, and neurodegenerative processes leading to disorders of the central and sensory-motor systems.
Our fundamental research is the ground for the development of innovative therapeutic (cell and gene therapy) and diagnostic (genetics and proteomics) strategies for hereditary retinal and optic nerve blindness, corneal damages, auditory neuropathy (deafness and tinnitus), somatosensory diseases (touch and pain), sleep disorders, cognition disorders (autism, schizophrenia, environmental stress) and neurodegenerative diseases (amyotrophic lateral sclerosis, multiple sclerosis, Alzheimer's disease).
Research, from the molecular level to the integrated system, is conducted using cutting-edge technical platforms (functional analysis, stem cell and organoids, neurogenetics, proteomics, biostatistics and epidemiology, photonic and electronic imaging). Our translational research is based on strong interactions with clinical services (neurology, ophthalmology, ENT). We benefit from the support of patient associations and interact constructively with industry.
Join the Institute for Neurosciences of Montpellier (INM) as a Junior Group Leader!
The INM, a leading research unit affiliated with Inserm and the University of Montpellier, is seeking talented junior researchers to develop cutting-edge neuroscience projects. We offer state-of-the-art facilities, opportunities for collaboration with established teams, and strong support for securing research funding. If you have a PhD (within the last 10 years) and are eager to advance your research career, apply by November 30th, 2024, to be considered for this exciting opportunity.

![]()
The INM is committed to the development of eco-responsible research
RECENT ARTICLES
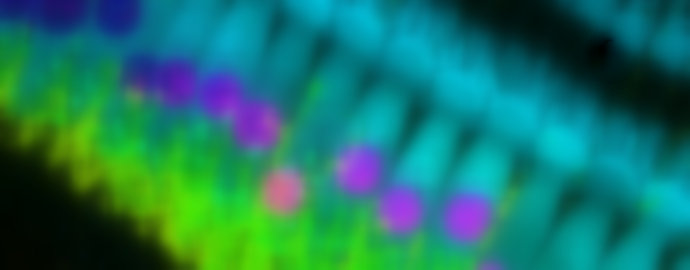
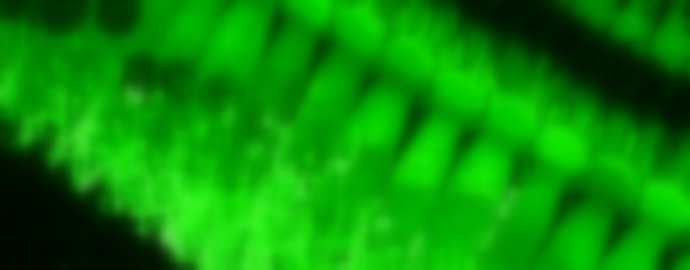
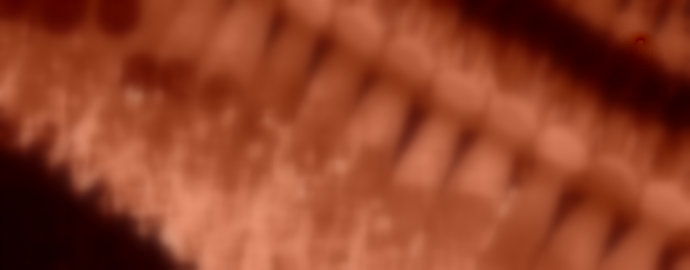
Identification of novel roles for ion channels in RPE function and homeostasis
Using CRISPR/Cas9 to mediate allele-specfic knockout as a treatment for autosomal dominant retinitis pigmentosa
New lipophenols for the etiological treatment of hereditary macular dystrophies
A new gene involved in the age-related hearing loss
Identification of a new gene causing both dominant and recessive forms of the most frequent blinding inherited disorder: retinitis pigmentosa